Study: Heart Failure Patients Demonstrate High Adherence with Passive Monitoring & Weight Measurements
Heart failure (HF) has become a common use case for care-at-home models. Remote monitoring yields deeper insight into disease progression and its associated symptoms, allowing care teams to titrate medications quickly and observe the effects of lifestyle changes in real-time.
In order to better understand engagement with technology among HF patients, the Current Health Clinical Research Team studied the adherence to four remote monitoring measures of participating patients across three care-at-home programs within US health systems.
The study revealed that patients across programs had the highest adherence with the continuous passive wearable device and the bluetooth-connected weight scale.
Read the Full Article at the Journal of the American College of Cardiology
Adherence Across 4 Program Elements
As part of the HF programs, patients were asked to wear the Current Health continuous monitoring device, submit daily weight and blood pressure readings, and/or complete daily symptom surveys on a provided tablet.
Adherence was derived from tasks and wear time completed versus prescribed.
154 admissions were evaluated and the mean age of study participants was 70 (+ -11.6 years old). The median monitoring duration was 14 days (IQR 7-36) with 54,125 total hours of data transmitted.
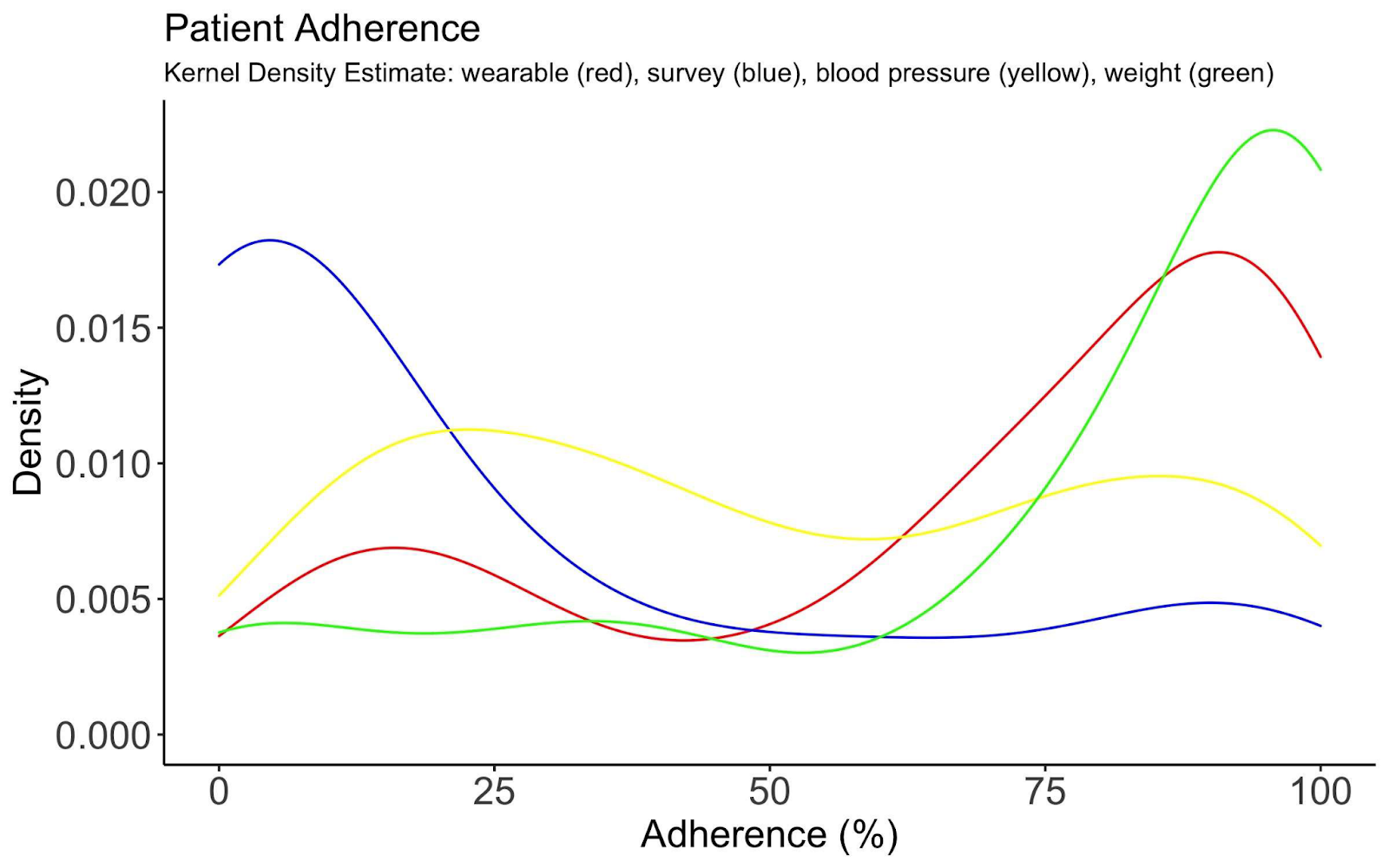
The highest adherence was with wearables and weight:
- Wearable: 77.5%
- Weight: 89%
Adherence regarding blood pressure monitoring and participating in patient surveys was lowest:
- Blood Pressure Cuff: 44%
- Surveys: 11%
While this study didn’t answer why these adherence trends were the case, the analysis from Rhiannon Berry and Philip Keeling in the article” Compliance with Telemonitoring in Heart Failure. Are Study Findings Representative of Reality?: A Narrative Literature Review” suggests a correlation between patient burden over time and reduced compliance:
“Several studies reported a decline in compliance with an increasing number or frequency of measurements required from patients. This suggests that the more patients are expected to engage and interact with telemonitoring, the less compliant they may be. Interestingly, these findings are aligned with those for medication adherence in HF patients, where the risk of poor medication adherence is significantly greater with a higher number of total daily medications. Like medication taking, telemonitoring requires compliance over a long time from HF patients. However, telemonitoring may often require the recording and submission of multiple vital parameters, which may be more time consuming for patients than taking medication.”
Targeted Engagement Strategies
Care-at-home program leaders should be aware that adherence may vary between measures. Clinicians must weigh data richness, with the burden of collection, to maximize clinical utility and adherence.
To address lower adherence with blood pressure readings and symptom surveys, care-at-home programs aimed at managing HF may benefit from targeted engagement or accountability around these measures to improve data completeness. The adherence divide also highlights the importance of patient education focused on the devices and clinical measurements. Patients should receive instruction about both how to complete readings and why each reading is important to their health and care plan.
Program leaders should also note that remote monitoring may not be a good fit for some, regardless of measures, so careful patient selection is critical.
Watch how the HF care-at-home program at Baptist Health helped Jenny return to the things she loves most.


![[Webinar Recording]This Way Home: Top 10 Predictions for Care at Home in 2025](https://www.currenthealth.com/wp-content/uploads/2025/01/DSG-846-JAN-WEBINAR-LINKEDIN-16_9-AD2-P2.jpg)